Abstract
Background: children in Africa are mainly affected by epilepsy. This study describes the clinical and paraclinical profiles of epileptic children followed at the Neuro-Psychopathological Center of the University of Kinshasa (CNPP/Unikin). Method: a descriptive cross-sectional study analyzed the files of patients aged ≤ 15 years old admitted to the pediatric neurology unit of the CNPP/Unikin, from December 2015 to December 2020. The variables of interest were sociodemographic, clinical, and evolutionary. Excel 2010 and SPSS version 20.0 were used to manage the data. Results: 118 files of children (70 boys and 48 girls) were collected; 40.7% were between 11 and 15 years old. The mean (SD) age was 8.2 (4.1) years. Sixty percent of admissions were due to epilepsy. Forty-seven (39.8%) patients had idiopathic epilepsy. The majority (83.1%) of seizures is generalized and tonic-clonic seizure is predominant (64.4%). Comorbidities were dominated by neurodevelopmental disorders (8%). Nutritionally, hypocalcaemia (51.7%), hypomagnesaemia (16%) and hypokalemia (1.7%) were observed. Abnormalities during pregnancy and childbirth (23.7%) were the most common etiological factors. The seizures outcome under treatment was characterized, in general, by regression (64.4%). Conclusion: epilepsy is the leading cause of admission in CNPP/Unikin neuropediatric unit, with increasing rates. Nutritional disorders, abnormalities during pregnancy, and childbirth are the dominant etiological factors in these children living with epilepsy. Therefore, health policies must be deeply reassessed, Sub-Saharan Africa, to improve the management and prevention of both epilepsy and identified etiological factors.
Keywords
Clinic, Epilepsy, Neuropediatry, Paraclinic, Sub-Saharan Africa
1. Introduction
Epilepsy is one of the most common neurological diseases in the world
. Each year, it is diagnosed in 2.4 million people, and nearly 80% of these people with epilepsy are thought to live in developing countries
| [2] | Sayers J. The world health report 2001 — Mental health: new understanding, new hope. Bull World Health Organ. 2001; 79(11): 1085. PMCID: PMC2566704. |
[2]
. Generally speaking, regardless of age and when only active epilepsy is taken into account, the prevalence of epilepsy in sub-Saharan Africa varies between 7 and 14.8‰
| [3] | Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza Mwesige A, Ae-Ngibise K et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross- sectional and case control studies. Lancet Neurol. 2013; 12(3): 253- 263. |
[3]
. The number of new cases of epilepsy in this part of Africa is increasing, ranging from 63 to 158 per 100,000 inhabitants per year
| [3] | Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza Mwesige A, Ae-Ngibise K et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross- sectional and case control studies. Lancet Neurol. 2013; 12(3): 253- 263. |
[3]
. This region of Africa also has very high epilepsy prevalence rates ranging from 5.2 to 74 per 1,000 people depending on the methods used and the regions
| [4] | Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238. |
[4]
and epilepsy mainly affects children
| [5] | Dadah Samy Mohamed Lemine, Ben-Adji Djibrilla Wazir, Basse Anna Modji, Sow Adjaratou Dièynaba, Sene Marième Soda, Faye Mouhameth, Cisse Ousmane, Ba El Hadji Makhtar, Seck Lala Bouna, Diagne Side Ngor, Touré Kamadore, Diop Amadou Gallo, Ndiaye Mouhamadou Mansour, Ndiaye Moustapha. Epilespie of the child and adolescent in Senegal. African Journal of Neurological Sciences 2015 (33); 1: 3-9. |
[5]
. A wide variability in the distribution of epileptic seizures, depending on age and environmental factors, is known worldwide
| [4] | Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238. |
[4]
. In sub-Saharan Africa, epileptic seizures are frequent, accounting for up to 18.3% of pediatric emergency consultations
| [6] | Idro R, Gwer S, Kahindi M, Gatakaa H, Kazungu T, Ndiritu M, Maitland K, Neville BG, Kager PA, Newton CR. The incidence, aetiology and outcome of acute seizures in children admitted to a rural Kenyan district hospital. BMC Pediatr. 2008; 8: 5. |
[6]
. Their incidence is estimated at 423/100,000 inhabitants per year for children aged 0-13 and 879 for children under 5
| [6] | Idro R, Gwer S, Kahindi M, Gatakaa H, Kazungu T, Ndiritu M, Maitland K, Neville BG, Kager PA, Newton CR. The incidence, aetiology and outcome of acute seizures in children admitted to a rural Kenyan district hospital. BMC Pediatr. 2008; 8: 5. |
[6]
. The exact incidence or prevalence of epileptic seizures or of the most frequent neuropediatric conditions, notably epilepsy, is not known in the city of Kinshasa or in the whole of the Democratic Republic of Congo. This situation is due, among other things, to an obvious lack of epidemiological studies
| [7] | Kaputu-Kalala-Malu Célestin et al. Epilepsy and acute seizures in children in sub-Saharan Africa: challenges and hopes. Pan African Medical Journal. 2016; 23: 58. |
[7]
. This study aims to present an overview of epileptic seizures in a neuro-pediatric hospital population in Kinshasa, by describing the clinical and paraclinical profile of epileptic seizures in children treated for epilepsy at the Neuro-Psychopathological Center of the University of Kinshasa, DRC.
2. Materials and Methods
2.1. Nature, Period and Area of Study
We conducted a cross-sectional study in the outpatient service, the Neuropediatric Unit, of the Neuro-Psychopathological Center of the University of Kinshasa. It focused on records of patients aged 15 years or younger admitted to this unit, from December 2015 to December 2020, for epileptic seizures. The diagnosis of epilepsy was electro-clinical, based on clinical data sometimes supported by epileptiform activity on EEG (electroencephalography). These children were admitted in the critical or intercritical phase. The electroencephalographic recordings (all intercritical) were made by two technicians and interpreted by the physicians (senior neuropsychiatric assistant and epileptological neuropsychiatrist) under the supervision of the professors (of neuropediatry and of developmental neuropsychiatry).
2.2. Study Population
The study involved the records of children regularly followed for epilepsy for at least 2 years in the CNPP/Unikin pediatric neurology unit.
Inclusion criteria: all patients with known epilepsy, aged 15 or under, treated with an antiepileptic and regularly followed for at least 2 years in the CNPP/Unikin pediatric neurology unit, were included.
Non-inclusion criteria: patients who did not an electroencephalogram or whose files were incomplete were excluded.
2.3. Data Collection and Parameters of Interest
For all included files, our variables of interest were sociodemographic: age and sex of the child; personal and family history: course of pregnancy and delivery, neonatal jaundice, infection or affection in childhood, notion of epilepsy and/or febrile convulsions, compliance with vaccination schedule, psychomotor development; electro-clinical and clinical investigation completed by neuropsychiatric evaluation with DSM IV /MINI-KID
| [8] | Lecrubier Y, Weiller E, Hergueta T, Amorim P, Bonora L. I, J. P. Lépine J. P. (INSERM-PARIS, FRANCE) / Sheehan D, Janavs J, Baker R, Sheehan K. H., Knapp E., Sheehan M. (University of South Florida-TAMPA, USA). Mini International Neuropsychiatric Interview. Version 5.0.0 / DSM-IV / current (August 1998). |
[8]
. These data are specified on the collection form: epidemiological and sociodemographic data (age and sex of the child); existence of parental consanguinity; geographical origin of the child and occupation of the parents; abnormalities during pregnancy and difficulty in childbirth, abnormalities in psychomotor development; personal or family history of epilepsy; clinical data (type of seizure and other associated neurosomatic signs) and paraclinical data [intercritical electroencephalographic (EEG) recording, blood ionogram, Magnetic Resonance Imaging (MRI) or cerebral CT scan whenever possible]; treatment and clinical course of seizures.
2.4. Operational Definitions
The parental consanguinity was defined as marriage between: a) first cousins; related within 1
er degree, b) second cousins. The clinical course of seizures was assessed on the basis of weekly seizure frequency, and could be favorable (reduction in seizure frequency) or unfavorable (clinical status quo or increase in seizure frequency). The classification of epileptic seizures and epilepsy was made in accordance with the recommendations of the International League Against Epilepsy
| [9] | Cambier J, Masson M, Dehen H. Abrégés de Neurologie. 11th edition, Masson, Paris, 2000, pp. 181-206. |
[9]
.
2.5. Statistical Analysis
Data entry and management were carried out using Excel 2010. Statistical analysis was performed using SPSS software version 20.0. Univariate analysis, where means, medians and standard deviations were calculated to describe quantitative variables. Frequencies were calculated for all categorical variables of interest.
2.6. Ethical Considerations
The protocol for this study was approved by the Ethics Committee of the School of Public Health of the University of Kinshasa, under number: ESP/CE/013/2022. Confidentiality and anonymity were respected.
3. Results
3.1. Study Population
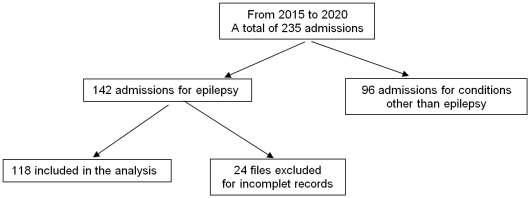
Over 5 years, we recorded 238 cases of children admitted to pediatric neurology unit, including 142 cases of epileptic seizures, a frequency of 59.7%. The number of epileptic seizures recorded was 118; the remainder (24) were incomplete;
figure 1.
Figure 1. Files selection process.
3.2. Socio-epidemiological Data
The average age of the children was 8.2 ± 4.1 years. Youngest aged 1.5 and oldest aged 15. Children aged 11 years or older (40.6%) and male (59.3%) were the most represented. The age groups of 0-5 years and 6-10 years represented respectively 31.4 and 28% of the series. The sex ratio was 3 boys for 2 girls.
3.3. Clinical Data
Table 1 below shows the distribution of children according to their clinical data. Generalized seizures predominated. The inaugural seizure occurred in the majority of subjects (54.2%) at an age less than or equal to 2 years, and on average at 3.3(3.2) years. Most (78%) of these children had no family history of epilepsy. Parental consanguinity was noted to 10 (8.3%) children. The clinical evolution of seizures was generally (64.4%) favorable.
Table 1. Distribution of children's clinical data.
Variables | N (%) |
Age of onset of 1st crisis | ≤ 2 years | 64 (54,2) |
> 2 years | 54 (45,8) |
Epilepsy in the family | No | 92 (78,0) |
Yes | 26 (22,0) |
The time between onset of last crisis and admission to CNPP | ≤10 days | 63 (53,4) |
>10 days | 55 (46,6) |
Sickly child in 1st childhood (early childhood infections) | No | 90 (76,2) |
Yes | 28 (23,7) |
Pregnancy and childbirth abnormalities. n=28 (23.7%) | Perpartal asphyxia | 13 (11) |
Resuscitation at birth | 11 (9,3) |
Neonatal jaundice | 5 (4,2) |
Comorbidities | No | 77 (65,2) |
Yes | 41(34,8) |
Clinical type of seizures | Generalized seizures | 98 (83,1) |
Partial (or localized) seizures | 20(16,9%) |
Clinical form of seizures | Tonic-clonic | 77(65,3) |
Myoclonic | 9(7,6) |
Atone | 8(6,8) |
Complex | 7(5,9) |
Absence | 7(5,9) |
Tonic | 5 (4,2) |
Clonic | 5(4,2) |
Etiological types of seizures | Idiopathic crisis | 47(39,8) |
Unclassifiable crisis | 33 (28) |
Non-idiopathic crisis | 24 (20,3) |
Febrile convulsion | 13 (11) |
Seizure outcome under treatment | | |
Favorable. n=76 (64.4%) | Complete remission | 45(38,1) |
Partial remission | 31(26,3) |
Unfavorable. n=42 (35.6%) | Status quo | 31(26,3) |
Worsening | 11(9,3) |
3.4. Comorbidities and Paraclinical Data
Table 2 below shows the distribution of comorbidities and paraclinical data. The comorbidities were found in 41 children (34.8%), and were dominated by neurodevelopmental delay in 8% of cases. Two of these children had a combination of comorbidities: one with neurodevelopmental delay and polydactyly, and another with craniofacial dysmorphia associated with neurocognitive deficit. EEG was performed in all 118 children (100%). As shown in this
Table 2, EEG was epileptogenic in 41 (34.7%) subjects; these were mainly (26.3%) generalized or diffuse epileptogenic grapho elements. Cerebral CT scan or MRI were performed in 65 children (55.1%) and were abnormal in 25 (38.5%). The main abnormalities found were hydrocephalus in 9 cases (13.3%); intracerebral cyst in 6 cases (9.2%); cerebro-cerebellar atrophy in 4 cases (6.2%); cerebral ischemia in 3 cases (4.6%); glioma in 2 cases (3.1%) and hemimegalencephaly in 1 case (1.5%).
Table 2. Distribution of comorbidities and of Paraclinical data.
Variables | n (%) |
Types of comorbidities n= 41(34,8%) | Neurodevelopmental delay | 9(7,6) |
Craniofacial dysmorphia | 6(5) |
ADHD | 4(3,4) |
Malformation (tumor) | 4(3,4) |
Ligament hyperlaxity | 3(2,5) |
Sickle cell disease | 2(1,7) |
Motor disability | 2(1,7) |
Extremity anomalies (polydactyly) | 2(1,7) |
ASD | 1(0,8) |
Paraclinical data |
EEG results | Non epileptogenic | 77(65,2) |
Epileptogenic | 41(34,7) |
Diffused | 31(26,3) |
Located | 10 (8,4) |
Epileptogenic EEG profile | Tips | 23(19,5) |
Tip-wave | 30(25,4) |
Poly tips | 27(22,9) |
Poly tip-wave | 7(5,9) |
Cerebral MRI / CT scan results. (Structural brain abnormalities) n=25 (21.2%) | Hydrocephalus | 9(13,3) |
Intracerebral cyst | 6(9,2) |
Cerebro-cerebellar atrophy | 4(6,2) |
Cerebral ischemia | 3(4,6) |
Glioma | 2(3,1) |
Hemimegalencephaly | 1(1,5) |
Blood ionogram | Hypocalcemia | 61(51,7) |
Hypomagnesemia | 19(16) |
Hypokalemia | 2(1,7) |
ADHD = Attention Deficit and Hyperactivity Disorder ASD=Autistic Spectrum Disorder
MRI=Magnetic Resonance Imagery EEG = electroencephalography
4. Discussion
Admission for epileptic seizures is a permanent reality in Congolese neuropediatric. In this study, the average age of children at the time of inaugural seizures was 3.3±3.2 years, that of patients on admission was 8.7 ± 4.1 years, with children aged 11 years or over (40.7%) being the most represented, and the 60% frequency of admission for epileptic seizures in the pediatric neurology consultation at CNPP/Unikin, are in line with the precocity of seizure onset. According to the literature, over 60% of epileptic seizures occur before the age of 20
| [4] | Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238. |
[4]
. A Senegalese study
| [10] | Ndiaye M, Sarr M, Mapoure Y, Diouf FS, Toure K, Sow AD et al. Epilepsy in the Senegalese neuro-pediatric context. Rev Neurol. 2008; 164(2): 162-168. |
[10]
and a Congolese study
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[11]
observed mean patient ages of 6.3 and 8.5 years respectively, which are comparable to that observed in this series. The predominance of males (59.3%), with a sex ratio of 3 males for 2 females, found in this study is similar to that found in the literature. Several African studies have observed the male predominance of epileptic seizures
| [3] | Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza Mwesige A, Ae-Ngibise K et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross- sectional and case control studies. Lancet Neurol. 2013; 12(3): 253- 263. |
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
| [12] | Hutu K, Kaputu K, Mukeba K, Okitundu LEA, Kayembe K. Retrospective analysis of 210 cases of epileptic seizure at the Centre Neuro-Psychopathologique de Kinshasa. Ann. Afr. Med, Vol. 3, N° 3, June 2010. 505-5011. |
| [13] | Ndong MEY, Ndiaye M, Fall M. Idiopathic epilepsies in children: about 186 children followed for 3 years at CHU de Fann (Dakar- Senegal). Rev Neurol. 2016; 172(1): 55. |
[3, 11-13]
. Although it was not encountered by Hurst and Reef in South Africa
| [14] | Hurst LA, Reef HE. Neuropsychiatric disorders in Bantu. S Afr Med J. 1961; 35: 750-754. |
[14]
and by Orly and al. in Uganda
| [15] | Orly J. Epilepsy in Uganda (rural) A study of eighty- three cases. Afr J Med Sci 1970; 1: 155- 160. |
[15]
, this male preponderance would relate not only to social behavior in the African environment, which would lead to under-reporting of epileptic seizures in girls
| [16] | Sarfaty, J. " Épilepsie et structuration psychique de l'enfant ", Contraste, vol. 38, no. 2, 2013, pp. 143-154. |
[16]
, as well as a possible neurobiological difference between male and female, resulting in differentiated responses to brain lesions
| [5] | Dadah Samy Mohamed Lemine, Ben-Adji Djibrilla Wazir, Basse Anna Modji, Sow Adjaratou Dièynaba, Sene Marième Soda, Faye Mouhameth, Cisse Ousmane, Ba El Hadji Makhtar, Seck Lala Bouna, Diagne Side Ngor, Touré Kamadore, Diop Amadou Gallo, Ndiaye Mouhamadou Mansour, Ndiaye Moustapha. Epilespie of the child and adolescent in Senegal. African Journal of Neurological Sciences 2015 (33); 1: 3-9. |
[5]
. The disparity with the South African and Ugandan studies is thought to be due to selection bias.
In this study, the average delay between consultation of patients at the CNPP/Unikin and the onset of the last crisis was 1.6±1.2 months. A high frequency (47%) of children with this delay of more than 10 days was observed. The type of seizure most frequently encountered in this study was the generalized seizure (83.1% of cases), with a predominance of the tonic-clonic form (64.4% of cases). This result corroborates the observations of several other Congolese and African authors
| [7] | Kaputu-Kalala-Malu Célestin et al. Epilepsy and acute seizures in children in sub-Saharan Africa: challenges and hopes. Pan African Medical Journal. 2016; 23: 58. |
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[7, 11]
. This may be explained by: a) the fact that epileptics in sub- Saharan Africa still do not have easy access to modern treatment due, among other things, to the mystico-religious and cultural beliefs that still surround this disease
| [17] | Wilmshurst JM, Burman R, gaillard WD, cross JH. Treatment of infants with epilepsy: common practices around the word. Epilepsia. 2015; 56(7): 1033-1046. |
[17]
; b) the spectacular nature of the generalized tonic-clonic crises that forces the family to consult for their child, and c) the lack of awareness among the population of other manifestations and forms of non-convulsive seizures, which would also explain the low frequency of absence seizures in this study as in other African studies
| [5] | Dadah Samy Mohamed Lemine, Ben-Adji Djibrilla Wazir, Basse Anna Modji, Sow Adjaratou Dièynaba, Sene Marième Soda, Faye Mouhameth, Cisse Ousmane, Ba El Hadji Makhtar, Seck Lala Bouna, Diagne Side Ngor, Touré Kamadore, Diop Amadou Gallo, Ndiaye Mouhamadou Mansour, Ndiaye Moustapha. Epilespie of the child and adolescent in Senegal. African Journal of Neurological Sciences 2015 (33); 1: 3-9. |
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[5, 11]
. This situation shows the major challenge not only of diagnosis, but also of correct and early management of epilepsy in Sub-Saharan African countries. Various socio-cultural constraints and beliefs are therefore permanent and obvious limitations at the root of the delay in referral, in the delay in diagnosis and in the treatment of patients
| [7] | Kaputu-Kalala-Malu Célestin et al. Epilepsy and acute seizures in children in sub-Saharan Africa: challenges and hopes. Pan African Medical Journal. 2016; 23: 58. |
[7]
.
We noted a high frequency (45.8%) of idiopathic seizures, in line with the literature
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[11]
. In sub-Saharan Africa, the low level of household income would not allow access to expensive means of investigation
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[11]
. However, the frequency of partial seizures underlines the importance of morphological explorations of the brain in these children. However, MRI or CT brain scans, the examinations of choice for morphological exploration of the brain in children with epilepsy, were carried out in this series in 65 children (55.1%), and were abnormal in 25 (38.5%). Generally speaking, in developing countries, due to the lack of health care facilities and the multiplicity of etiological factors involved in epileptic seizures, a specific etiology is identified in only 40% of epileptic seizure cases
| [18] | Preux PM, Druet-Cabanac M. Epidemiology and etiology of epilepsy in sub-saharan Africa. Lancet Neurol. 2005; 4(1): 21-31. |
[18]
.
Comorbidities were found in 41 children (34.8%), and were dominated by neurodevelopmental delay in 8% of cases. Two of these children even had a combination of comorbidities. In a child with epilepsy, an epileptic seizure is often just the tip of the iceberg, or part of a more complex set of manifestations. It is often these comorbidities that impair the quality of life of children living with epilepsy. But in developing countries, due to poor infrastructure and limited paraclinical means of investigation, these comorbidities are often ignored or go unnoticed.
Concerning the etiology of epileptic seizures in this series, abnormalities of pregnancy and delivery were observed in 28(23.7%) children: 13(11%) suffered from perpartal asphyxia, 11(09.3%) were resuscitated at birth and 5(4.2%) experienced neonatal jaundice. In a Senegalese study, 14.4% of children were resuscitated at birth
| [10] | Ndiaye M, Sarr M, Mapoure Y, Diouf FS, Toure K, Sow AD et al. Epilepsy in the Senegalese neuro-pediatric context. Rev Neurol. 2008; 164(2): 162-168. |
[10]
. The high risk of epileptic seizures in a maturing brain may be exacerbated, in our environment, by poor monitoring of pregnancy and delivery, malnutrition, infections and post-traumatic stress
| [19] | Mampunza MM, Matonda MM, Lelo M, Ngo Mbok, Babong CL, Mpundu J. Post-traumatic stress disorder and epilepsy: Experience of the "Telema" Mental Health Center in Kinshasa. Ann Afr Med. 2007; 1 (1): 59-63. |
[19]
. Better management of these crises linked to abnormalities in pregnancy and childbirth must necessarily involve psychosocial support, prevention and early curative treatment of brain damage caused by intracranial aggression
| [12] | Hutu K, Kaputu K, Mukeba K, Okitundu LEA, Kayembe K. Retrospective analysis of 210 cases of epileptic seizure at the Centre Neuro-Psychopathologique de Kinshasa. Ann. Afr. Med, Vol. 3, N° 3, June 2010. 505-5011. |
[12]
.
Ionic disorders, with the preponderance of hypocalcemia observed in this study, suggest a close link, in sub-Saharan Africa, between epilepsy and nutritional factors. Epilepsy may be a cofactor in the onset of malnutrition, or malnutrition may favour the onset of epilepsy or epileptic seizures
| [20] | Sabrina Crépin, Bertrand Godet, Benoît Chassain, Pierre-Marie Preux, Jean-Claude Desport, Malnutrition and epilepsy: complex links, Nutrition Clinique et Métabolisme, Volume 22, Issue 2, 2008, Pages 88-95. |
[20]
. Some authors
| [21] | Richard Hackett, Thomas Iype, Malnutrition and childhood epilepsy in developing countries, Seizure, Volume 10, Issue 8, 2001, Pages 554-558. |
| [22] | Stella L. Volpe, Joan I. Schall, Paul R. Gallagher, Virginia A. Stallings, A. G. Christina Bergqvist, Nutrient Intake of Children with Intractable Epilepsy Compared with Healthy Children, Journal of the American Dietetic Association, Volume 107, Issue 6, 2007, Pages 1014-1018. |
[21, 22]
have demonstrated the role of nutrition and nutritional status in the onset of epilepsy: in the case of energy and protein deficiencies, or deficiencies in mineral salts, vitamins or trace elements. Conversely, the role of epilepsy in the onset of undernutrition has also been proposed
| [21] | Richard Hackett, Thomas Iype, Malnutrition and childhood epilepsy in developing countries, Seizure, Volume 10, Issue 8, 2001, Pages 554-558. |
[21]
: the weight of food prohibitions and social exclusions with regard to children with epilepsy may play a role. In Africa, therefore, malnutrition and epilepsy are sometimes associated, and can form a vicious circle
| [20] | Sabrina Crépin, Bertrand Godet, Benoît Chassain, Pierre-Marie Preux, Jean-Claude Desport, Malnutrition and epilepsy: complex links, Nutrition Clinique et Métabolisme, Volume 22, Issue 2, 2008, Pages 88-95. |
[20]
.
Apart from consanguinity, which remains rare (8.5%) in this series, infections in early childhood (23.7%), a family history of epileptic seizures (22%) and structural cerebral anomalies (21.2%) are the etiological factors most frequently found both in the literature
| [4] | Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238. |
| [11] | Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10). https://doi.org/10.5281/hsd.v22i10.3023 |
[4, 11]
and in this study. Some authors report a very high frequency of family antecedents, especially in the first degree
| [23] | Mukalay M, Kalenga MK, Dramaix M, Hennart Ph, Kabyla I, Donnen Ph. Prevalence and determinants of malnutrition in children under 5 years of age in the Bongonga district of Lubumbashi. Ann Afr Med. 2009; 3 (1): 346- 354. |
[23]
. Others, however, report weak associations
| [4] | Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238. |
| [24] | EL Gengaihy ME, Wasif SM. Epidemiological study of epilepsy in Egypt. Neurologie tropicale. ED. AUPELF-UREF. John Libbey Eurotext, Paris 1993, pp. 39-45. |
[4, 24]
. Parental consanguinity and a family history of epileptic seizures are suggestive of a genetic predisposition. However, there is little consensus in the literature as to the presence of a family history of epilepsy in any individual with epilepsy.
5. Conclusion
Admissions for epileptic seizures account for 60% of pediatric neurology consultations at CNPP/Unikin. A large number of these seizures are generalized tonic-clonic, early-onset and predominate in boys and children aged 11 to 15. Etiological factors of secondary epilepsy are dominated by nutritional disorders and abnormalities in pregnancy and childbirth. This study highlights that the health policies must be deeply reassessed, in Sub-Saharan Africa, to improve the management and prevention of both epilepsy and identified etiological factors.
State of Knowledge on the Subject
1. Epileptic seizures, such as epilepsy, are increasingly common in African pediatric settings.
2. They are associated with comorbidities that often go unnoticed.
3. Food bans and social exclusion from children with epilepsy can lead to malnutrition of these children and thus worsen their health.
4. The relationship between malnutrition, pregnancy abnormalities, comorbidities and epileptic seizures is not often deepened in Africa.
5. The management of both epileptic seizures and epilepsy is often inadequate in Africa; the lack of qualified personnel, under-equipment and cultural influence are often mentioned to explain this dramatic situation.
Contribution of this study to knowledge
1. This study enriches the epidemiology and clinic of childhood epileptic seizures in Africa.
2. She analyzed not only the clinical aspects, but also the etiological factors of epileptic seizures, which were found to be dominated by blood ionogram disorders (nutritional disorders), pregnancy and childbirth abnormalities, before paying particular attention to the evolutionary aspect.
3. She highlighted the need to deepen the real impact of nutritional factors, pregnancy and childbirth abnormalities in children with epilepsy in Africa.
Abbreviations
ADHD | Attention Deficit and Hyperactivity Disorder |
ASD | Autistic Spectrum Disorder |
CNPP/Unikin | Neuro-Psychopathological Center of the University of Kinshasa |
CT | Computed Tomography |
DRC | Democratic Republic of Congo |
DSM IV | Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition |
MINI-KID | Mini-International Neuropsychiatric Interview for Children and Adolescent |
EEG | Electroencephalography |
MRI | Magnetic Resonance Imagery |
Author Contributions
Victor Hutu Kabamba: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Alphonsine Ntumba Lukusa: Conceptualization Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Philippe Ntalaja Kabuayi: Data curation, Formal Analysis, Methodology, Software, Writing – original draft
Sylvie Ntumba Mbombo: Conceptualization, Formal Analysis, Methodology, Visualization, Writing – review & editing
Celestin Kaputu-Kalala-Malu: Conceptualization Formal Analysis, Methodology, Writing – original draft
Daniel Okitundu Luwa E-Andjafano: Conceptualization Formal Analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing
Funding
The authors did not receive any funding for this study.
Data Availability Statement
The database used and analyzed during the current study is available from the corresponding author and will available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization, Epilepsy. Fact sheet, 2024.
https://www.who.int/en/news-room/fact-sheets/detail/epilepsy
. Accessed 21 April 2024.
|
| [2] |
Sayers J. The world health report 2001 — Mental health: new understanding, new hope. Bull World Health Organ. 2001; 79(11): 1085. PMCID: PMC2566704.
|
| [3] |
Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza Mwesige A, Ae-Ngibise K et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross- sectional and case control studies. Lancet Neurol. 2013; 12(3): 253- 263.
|
| [4] |
Ngoungou EB, Quet F, Dubreuil CM, Marin B, Houinato D, Nubukpo P et al. Epidemiology of epilepsy in sub-Saharan Africa: a review of the literature. Sante. 2006; 16(4): 225-238.
|
| [5] |
Dadah Samy Mohamed Lemine, Ben-Adji Djibrilla Wazir, Basse Anna Modji, Sow Adjaratou Dièynaba, Sene Marième Soda, Faye Mouhameth, Cisse Ousmane, Ba El Hadji Makhtar, Seck Lala Bouna, Diagne Side Ngor, Touré Kamadore, Diop Amadou Gallo, Ndiaye Mouhamadou Mansour, Ndiaye Moustapha. Epilespie of the child and adolescent in Senegal. African Journal of Neurological Sciences 2015 (33); 1: 3-9.
|
| [6] |
Idro R, Gwer S, Kahindi M, Gatakaa H, Kazungu T, Ndiritu M, Maitland K, Neville BG, Kager PA, Newton CR. The incidence, aetiology and outcome of acute seizures in children admitted to a rural Kenyan district hospital. BMC Pediatr. 2008; 8: 5.
|
| [7] |
Kaputu-Kalala-Malu Célestin et al. Epilepsy and acute seizures in children in sub-Saharan Africa: challenges and hopes. Pan African Medical Journal. 2016; 23: 58.
|
| [8] |
Lecrubier Y, Weiller E, Hergueta T, Amorim P, Bonora L. I, J. P. Lépine J. P. (INSERM-PARIS, FRANCE) / Sheehan D, Janavs J, Baker R, Sheehan K. H., Knapp E., Sheehan M. (University of South Florida-TAMPA, USA). Mini International Neuropsychiatric Interview. Version 5.0.0 / DSM-IV / current (August 1998).
|
| [9] |
Cambier J, Masson M, Dehen H. Abrégés de Neurologie. 11th edition, Masson, Paris, 2000, pp. 181-206.
|
| [10] |
Ndiaye M, Sarr M, Mapoure Y, Diouf FS, Toure K, Sow AD et al. Epilepsy in the Senegalese neuro-pediatric context. Rev Neurol. 2008; 164(2): 162-168.
|
| [11] |
Sounga Bandzouzi, P. E. G., Mpandzou, G. A., Diatewa, J. E., Motoula-Latou, D. H., Ngassaki, S., Mialoudama, C., Obondzo-Aloba, K. L., Bakoudissa, R., Mbourou Diouf, N., Mambila, G., Koubemba, C. G., & Ossou-Nguiet, P. M. (2021). Aspects Cliniques, Étiologiques et Thérapeutiques de l’Épilepsie du Nourrisson et de l’Enfant à Pointe-Noire. HEALTH SCIENCES AND DISEASE, 22(10).
https://doi.org/10.5281/hsd.v22i10.3023
|
| [12] |
Hutu K, Kaputu K, Mukeba K, Okitundu LEA, Kayembe K. Retrospective analysis of 210 cases of epileptic seizure at the Centre Neuro-Psychopathologique de Kinshasa. Ann. Afr. Med, Vol. 3, N° 3, June 2010. 505-5011.
|
| [13] |
Ndong MEY, Ndiaye M, Fall M. Idiopathic epilepsies in children: about 186 children followed for 3 years at CHU de Fann (Dakar- Senegal). Rev Neurol. 2016; 172(1): 55.
|
| [14] |
Hurst LA, Reef HE. Neuropsychiatric disorders in Bantu. S Afr Med J. 1961; 35: 750-754.
|
| [15] |
Orly J. Epilepsy in Uganda (rural) A study of eighty- three cases. Afr J Med Sci 1970; 1: 155- 160.
|
| [16] |
Sarfaty, J. " Épilepsie et structuration psychique de l'enfant ", Contraste, vol. 38, no. 2, 2013, pp. 143-154.
|
| [17] |
Wilmshurst JM, Burman R, gaillard WD, cross JH. Treatment of infants with epilepsy: common practices around the word. Epilepsia. 2015; 56(7): 1033-1046.
|
| [18] |
Preux PM, Druet-Cabanac M. Epidemiology and etiology of epilepsy in sub-saharan Africa. Lancet Neurol. 2005; 4(1): 21-31.
|
| [19] |
Mampunza MM, Matonda MM, Lelo M, Ngo Mbok, Babong CL, Mpundu J. Post-traumatic stress disorder and epilepsy: Experience of the "Telema" Mental Health Center in Kinshasa. Ann Afr Med. 2007; 1 (1): 59-63.
|
| [20] |
Sabrina Crépin, Bertrand Godet, Benoît Chassain, Pierre-Marie Preux, Jean-Claude Desport, Malnutrition and epilepsy: complex links, Nutrition Clinique et Métabolisme, Volume 22, Issue 2, 2008, Pages 88-95.
|
| [21] |
Richard Hackett, Thomas Iype, Malnutrition and childhood epilepsy in developing countries, Seizure, Volume 10, Issue 8, 2001, Pages 554-558.
|
| [22] |
Stella L. Volpe, Joan I. Schall, Paul R. Gallagher, Virginia A. Stallings, A. G. Christina Bergqvist, Nutrient Intake of Children with Intractable Epilepsy Compared with Healthy Children, Journal of the American Dietetic Association, Volume 107, Issue 6, 2007, Pages 1014-1018.
|
| [23] |
Mukalay M, Kalenga MK, Dramaix M, Hennart Ph, Kabyla I, Donnen Ph. Prevalence and determinants of malnutrition in children under 5 years of age in the Bongonga district of Lubumbashi. Ann Afr Med. 2009; 3 (1): 346- 354.
|
| [24] |
EL Gengaihy ME, Wasif SM. Epidemiological study of epilepsy in Egypt. Neurologie tropicale. ED. AUPELF-UREF. John Libbey Eurotext, Paris 1993, pp. 39-45.
|
Cite This Article
-
APA Style
Lukusa, A. N., Kabamba, V. H., Kabuayi, P. N., Mbombo, S. N., Malu, C. K., et al. (2024). Clinical and Paraclinical Profiles of Children Living with Epilepsy Admitted to Neuro-Psychopathological Center of Kinshasa. European Journal of Preventive Medicine, 12(6), 138-145. https://doi.org/10.11648/j.ejpm.20241206.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Lukusa, A. N.; Kabamba, V. H.; Kabuayi, P. N.; Mbombo, S. N.; Malu, C. K., et al. Clinical and Paraclinical Profiles of Children Living with Epilepsy Admitted to Neuro-Psychopathological Center of Kinshasa. Eur. J. Prev. Med. 2024, 12(6), 138-145. doi: 10.11648/j.ejpm.20241206.12
Copy
|
Download
AMA Style
Lukusa AN, Kabamba VH, Kabuayi PN, Mbombo SN, Malu CK, et al. Clinical and Paraclinical Profiles of Children Living with Epilepsy Admitted to Neuro-Psychopathological Center of Kinshasa. Eur J Prev Med. 2024;12(6):138-145. doi: 10.11648/j.ejpm.20241206.12
Copy
|
Download
-
@article{10.11648/j.ejpm.20241206.12,
author = {Alphonsine Ntumba Lukusa and Victor Hutu Kabamba and Philippe Ntalaja Kabuayi and Sylvie Ntumba Mbombo and Celestin Kaputu-Kalala Malu and Daniel Okitundu Luwa E-Andjafano},
title = {Clinical and Paraclinical Profiles of Children Living with Epilepsy Admitted to Neuro-Psychopathological Center of Kinshasa
},
journal = {European Journal of Preventive Medicine},
volume = {12},
number = {6},
pages = {138-145},
doi = {10.11648/j.ejpm.20241206.12},
url = {https://doi.org/10.11648/j.ejpm.20241206.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20241206.12},
abstract = {Background: children in Africa are mainly affected by epilepsy. This study describes the clinical and paraclinical profiles of epileptic children followed at the Neuro-Psychopathological Center of the University of Kinshasa (CNPP/Unikin). Method: a descriptive cross-sectional study analyzed the files of patients aged ≤ 15 years old admitted to the pediatric neurology unit of the CNPP/Unikin, from December 2015 to December 2020. The variables of interest were sociodemographic, clinical, and evolutionary. Excel 2010 and SPSS version 20.0 were used to manage the data. Results: 118 files of children (70 boys and 48 girls) were collected; 40.7% were between 11 and 15 years old. The mean (SD) age was 8.2 (4.1) years. Sixty percent of admissions were due to epilepsy. Forty-seven (39.8%) patients had idiopathic epilepsy. The majority (83.1%) of seizures is generalized and tonic-clonic seizure is predominant (64.4%). Comorbidities were dominated by neurodevelopmental disorders (8%). Nutritionally, hypocalcaemia (51.7%), hypomagnesaemia (16%) and hypokalemia (1.7%) were observed. Abnormalities during pregnancy and childbirth (23.7%) were the most common etiological factors. The seizures outcome under treatment was characterized, in general, by regression (64.4%). Conclusion: epilepsy is the leading cause of admission in CNPP/Unikin neuropediatric unit, with increasing rates. Nutritional disorders, abnormalities during pregnancy, and childbirth are the dominant etiological factors in these children living with epilepsy. Therefore, health policies must be deeply reassessed, Sub-Saharan Africa, to improve the management and prevention of both epilepsy and identified etiological factors.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinical and Paraclinical Profiles of Children Living with Epilepsy Admitted to Neuro-Psychopathological Center of Kinshasa
AU - Alphonsine Ntumba Lukusa
AU - Victor Hutu Kabamba
AU - Philippe Ntalaja Kabuayi
AU - Sylvie Ntumba Mbombo
AU - Celestin Kaputu-Kalala Malu
AU - Daniel Okitundu Luwa E-Andjafano
Y1 - 2024/11/26
PY - 2024
N1 - https://doi.org/10.11648/j.ejpm.20241206.12
DO - 10.11648/j.ejpm.20241206.12
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 138
EP - 145
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20241206.12
AB - Background: children in Africa are mainly affected by epilepsy. This study describes the clinical and paraclinical profiles of epileptic children followed at the Neuro-Psychopathological Center of the University of Kinshasa (CNPP/Unikin). Method: a descriptive cross-sectional study analyzed the files of patients aged ≤ 15 years old admitted to the pediatric neurology unit of the CNPP/Unikin, from December 2015 to December 2020. The variables of interest were sociodemographic, clinical, and evolutionary. Excel 2010 and SPSS version 20.0 were used to manage the data. Results: 118 files of children (70 boys and 48 girls) were collected; 40.7% were between 11 and 15 years old. The mean (SD) age was 8.2 (4.1) years. Sixty percent of admissions were due to epilepsy. Forty-seven (39.8%) patients had idiopathic epilepsy. The majority (83.1%) of seizures is generalized and tonic-clonic seizure is predominant (64.4%). Comorbidities were dominated by neurodevelopmental disorders (8%). Nutritionally, hypocalcaemia (51.7%), hypomagnesaemia (16%) and hypokalemia (1.7%) were observed. Abnormalities during pregnancy and childbirth (23.7%) were the most common etiological factors. The seizures outcome under treatment was characterized, in general, by regression (64.4%). Conclusion: epilepsy is the leading cause of admission in CNPP/Unikin neuropediatric unit, with increasing rates. Nutritional disorders, abnormalities during pregnancy, and childbirth are the dominant etiological factors in these children living with epilepsy. Therefore, health policies must be deeply reassessed, Sub-Saharan Africa, to improve the management and prevention of both epilepsy and identified etiological factors.
VL - 12
IS - 6
ER -
Copy
|
Download